
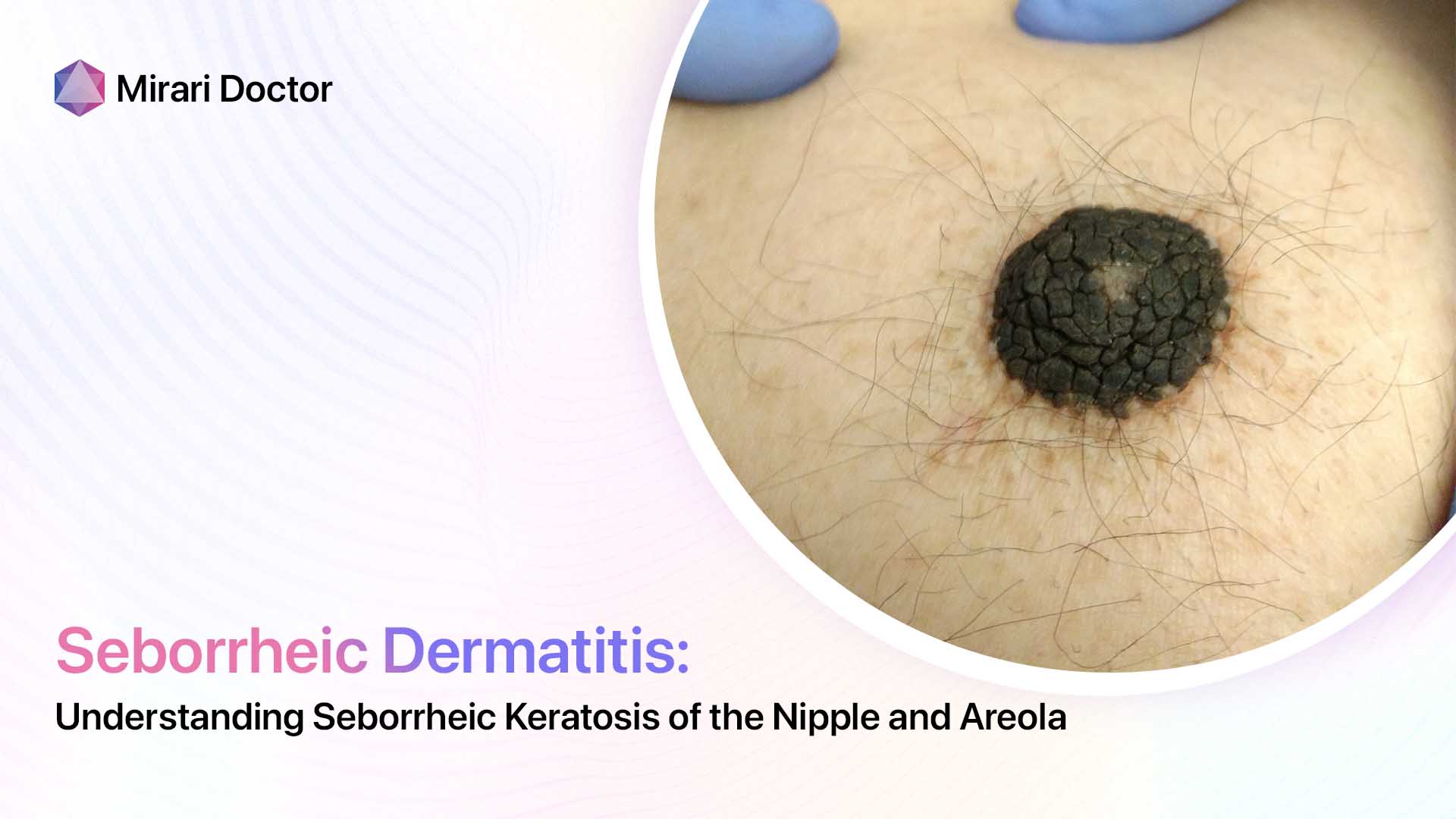
Seborrheic keratosis occurring on the nipple and areola is a relatively uncommon manifestation of this benign skin condition. However, awareness and recognition of seborrheic keratosis in this location is important to distinguish it from concerning mimickers.
Overview and Prevalence
Seborrheic keratosis is one of the most common benign skin tumors, affecting over 83 million Americans. Usually presenting as tan or brown warty growths, seborrheic keratoses can develop anywhere on the skin apart from the palms, soles, and mucous membranes.
The nipple and areola are infrequent sites for these lesions, with only a few case reports documenting seborrheic keratosis on the areola or seborrheic keratosis of the nipple. One study looking at nipple and areola biopsies over a 15-year period found seborrheic keratosis in only 0.4% of samples.
Clinical Features
Seborrheic keratoses on the nipple and areola tend to appear as sharply circumscribed, verrucous plaques ranging in color from tan to dark brown or black. They can be solitary or multiple, unilateral or bilateral. Pruritus is uncommon.
Some key characteristics help distinguish nipple/areola seborrheic keratoses from other benign and malignant growths in this location:
- Well-demarcated borders
- “Stuck-on” appearance
- Absence of nipple discharge or bleeding
- Lack of pain
- Slow growth over months to years

Mimickers
Seborrheic keratosis of the nipple or areola can be mistaken for other benign and malignant conditions. Critical entities in the differential diagnosis include:
Benign Mimickers
- Nevoid hyperkeratosis – presents as thicker, more diffuse nipple/areola plaque
- Epidermal nevus – onset in childhood; often unilateral
- Skin tags – soft, pedunculated growths
Malignant Mimickers
- Paget’s disease – eczematous changes, bleeding, itching, discharge
- Breast cancer – palpable mass, skin changes, nipple inversion/retraction
- Melanoma – history of changing mole; variegated colors
It is essential to recognize the warning signs of pagetoid spread of breast cancer and melanoma, which can be fatal if undetected. Any new nipple or areolar lesion warrants evaluation.
Pathogenesis
The etiology of seborrheic keratoses remains unclear. Proposed factors contributing to their development include:
- Accumulation of skin cell remnants – abnormal buildup of keratin debris and dead skin cells
- UV light exposure – solar radiation induces skin cell mutations
- Viral infection – human papillomavirus (HPV) may play a role
- Genetic changes – gene mutations lead to abnormal growth signaling
The nipple and areola have an abundance of pigment cells and hair follicles, skin appendages that may make them more prone to developing seborrheic keratoses. Hormones like estrogen are also hypothesized to stimulate these lesions.

Diagnosis
The diagnosis of a nipple or areolar lesion suspicious for seborrheic keratosis begins with a thorough clinical examination, noting features such as:
- Number of growths
- Size, shape, borders
- Color/pigmentation
- Surface texture
- Association with discharge, bleeding or itching
Imaging like mammography helps characterize nipple or skin changes related to an underlying breast mass.
Skin biopsy is required for definitive diagnosis, providing histological analysis of the lesional tissue. Under the microscope, seborrheic keratoses show characteristic findings of:
- Hyperkeratosis (thickened outer skin layer)
- Acanthosis (thickened lower skin layer)
- Horn cysts
- Basaloid cells
Treatments
Management of seborrheic keratosis on the nipple or areola centers around removal for cosmetic reasons or to exclude cancerous mimickers. Options include:
Medications
- Topical retinoids (tretinoin) – promote skin cell turnover
- Immunomodulators (imiquimod) – stimulate immune response against lesion
Procedures
- Cryosurgery – freezing with liquid nitrogen
- Curettage – scraping away growth
- Laser – destruction via carbon dioxide laser
- Surgical excision – elliptical cut-out of lesion
Complete lesion removal with clear margins helps prevent recurrence of nipple/areola seborrheic keratoses.
Prevention
Little is known about preventing seborrheic keratoses given uncertainties around their cause. Reasonable measures include:
- Sun protection with clothing and broad-spectrum SPF 30+ sunscreen
- Self-skin checks for any new or changing growths
- Routine skin cancer screenings by a dermatologist
Catching lesions early when they are small increases treatment success.

Prognosis
The prognosis for nipple or areola seborrheic keratosis is excellent, as they have no malignant potential. Recurrence rates are low after complete removal, especially if no atypical histological features are seen.
Patients should follow-up regularly with their healthcare provider for skin surveillance. Any symptoms like pain, bleeding, or itching warrant prompt reevaluation, even after prior treatment.
Key Takeaways
- Seborrheic keratosis on the nipple or areola is uncommon but important to recognize
- Distinguishing benign lesions like seborrheic keratosis from concerning mimics requires a high index of suspicion
- All new nipple/areola lesions deserve proper workup with imaging and biopsy
- Treatment involves medication or removal for diagnosis and cosmesis
- Regular self-skin checks are important even after treatment
Frequently Asked Questions
What causes seborrheic keratosis to occur on the nipple or areola?
The factors leading seborrheic keratoses to develop specifically on the nipple/areola are unclear but may involve sunlight, viruses, genetics, hormones, and accumulation of skin cell debris in hair follicles and pigment cells abundant in these areas. The nipple and areola have all the components to spur abnormal benign skin lesion growth.
How can you tell a seborrheic keratosis from Paget’s disease of the nipple?
While both may appear as nipple plaque or scaly patches, Paget’s disease has characteristic symptoms of itching, oozing, bleeding, and an underlying palpable mass from an associated breast cancer. Seborrheic keratoses are often asymptomatic apart from a “stuck-on” warty lesion. Skin biopsy is required for definitive diagnosis.
Can pregnancy cause nipple seborrheic keratoses to appear?
Pregnancy involves profound hormonal and skin changes that can trigger new benign skin growths around the areolae and nipples, including skin tags, moles, warts, and seborrheic keratoses. Self-breast and skin checks post-partum help identify any new worrisome lesions.
How can seborrheic keratosis be prevented from recurring after treatment?
Ensuring full lesion removal with clean margins during treatment helps prevent recurrent seborrheic keratoses in the same location. Ongoing sun protection, self-skin checks for new growths, and seeing a dermatologist regularly for skin cancer screening are also important for reducing recurrence risk.
What is the outlook for someone with a nipple seborrheic keratosis?
The prognosis for benign seborrheic keratoses confined to the nipple and areola is excellent. These lesions pose no threat of spreading or turning cancerous. However, patients still need monitoring for recurrence or any changes suggestive of new concerning pathology. Catching any abnormal nipple/skin changes early optimizes outcomes.
Conclusion
In summary, seborrheic keratosis involving the nipple and areola is rare but warrants appropriate diagnosis and management. Distinguishing benign lesions like seborrheic keratoses from mimickers with malignant potential is paramount. Treatment aims for complete lesion removal. Patients deserve education on self-skin checks and follow-up to monitor for recurrence and new lesions. While prognosis is reassuring, vigilant surveillance remains key.
Related articles


June 27, 2024
Seborrheic Dermatitis: Can Fluconazole Help?




June 19, 2024
Treating Seborrheic Dermatitis with Triamcinolone
June 19, 2024
Using Accutane to Treat Seborrheic Dermatitis


June 18, 2024
Can Itraconazole Help Treat Seborrheic Dermatitis?

June 18, 2024
Oregano Oil for Treating Seborrheic Dermatitis


Made in USA


600 North Bridge Rd #13-01
Parkview Square, Singapore 188788
Copyright © 2023 Mirari Doctor PTE. LTD.
All rights reserved.